The transgender community and its dermatologic needs are often unique and the scientific literature is sadly lacking in this group of patients. When we look at research, this is a common issue for many minority groups and the problem is well-recognised within the medical profession. Transgender patients face a number of healthcare barriers including discrimination and stigmatisation from others. Economic marginalisation is an issue facing most minority groups but for transgender patients, to add to the mix, there is often lack of access to healthcare professionals who are both knowledgeable and culturally sensitive to issues specific to the community. Information is sparse and the internet often becomes a primary source of information for those looking for answers.
There is a lack of representation of transgender skin issues in dermatology curriculums. Experience gained during a training programme varies wildly between doctors and can be dependent on the location in which postgraduate training took place. Dermatologists (and doctors in general) need to be inclusive and compassionate to our patients. Making assumptions regarding an individual’s gender identity, choice of pronoun, or sexual orientation are never appropriate. It is also hugely important to recognise that not all transgender patients who attend skin clinics want hormonal treatments or gender-affirming surgical procedures. The one thing I have learned in practice is simply to be respectful and ask your patient how they want to be addressed and what they want. It seems so simple yet can be done so badly and threaten to ruin the doctor-patient relationship.
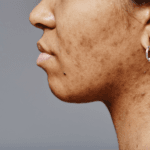
Dermatological conditions unique to this subgroup of patients include effects of hormonal-related therapy; transition can affect skin health. Transgender men taking androgens (such as testosterone) often experience worsening of acne affecting the face and back. This usually peaks at 6 months of treatment and starts to improve after about 12 months. Severe or scarring acne may require treatment with isotretinoin (Roaccutane). Adolescent transgender men who already have moderate to severe acne are those at highest risk of their skin flaring during hormonal treatment.
These patients may also require close monitoring of their liver blood tests (testosterone can cause raised liver enzymes and potentially so can isotretinoin). Administration of testosterone will also increase body hair and may lead to male-pattern hair loss (androgenetic alopecia). Of transgender men receiving androgen treatment on average for 10 years, 30% will develop scalp hair loss. Testosterone will alter body physique and overall body fat as well as prevent menstruation.
Conversely, therapy with oestrogen and anti-androgens in transgender women can also lead to specific skin changes including dryness, eczema and brittle nails as a result of reduced sebum or oil production. Whilst there will also be a reduction in body hair, additional measures such as laser treatment are likely to be needed to remove any remaining or unwanted hair. Feminising hormones will also result in breast development and redistribution of fat to create a female contour.
From an acne point of view, there are many things to consider, particularly in a male transgender patient (which is what triggered me to write this blog). Because of prescribing rules and pregnancy testing requirements, as a dermatologist I need to think about potential reproductive capacity and how best to sensitively address this in clinic. Done badly, without explaining context, this can alienate patients and prevent them seeking further interaction with healthcare. I don’t want this; the solution may be as simple as an “opt out of pregnancy prevention programme” in the UK and signing a waiver, but this needs to be explained and discussed.
For patients who are receiving testosterone and about to embark on isotretinoin, it requires honesty in saying that as doctors we don’t know if long-term remission from acne is possible. Long-term testosterone use may or may not continue to drive acne; we simply don’t have the data to definitively answer this question. Lastly, depressive symptoms and self-harm are more common in the transgender population than the cisgender population and there is also a relationship between acne and anxiety/depression. Patients need close monitoring for mood changes but treatment of acne may be life-changing in terms of confidence and self-esteem.
So when is the best time to seek help from a dermatologist? There are no hard and fast rules but if your acne is getting worse (you are noticing more spots or it is becoming more extensive, affecting multiple body sites, such as face, chest and back), failing to respond to over-the-counter skincare or prescription creams or tablets from your GP, or significantly starting to impact your mental health, self-esteem and body image, these are all signs you may need a skin specialist. Your NHS GP is able to refer you to your local NHS dermatology unit or if you have the financial means then you are able to directly access a private dermatologist who will be able to guide you through the options once they know a bit more about you and have the opportunity to examine your skin.